



Scientific and practical per-reviewed journal
Russian Journal of Cardiology is currently issued since 1996. It is official journal of the Russian Society of Cardiology (RSC).
Editor-in-Chief: Prof. Eugene V.Shlyakhto, Academician of Russian Academy of Sciences, President of RSC. FSBI «Almazov North-Western Federal Medical Research Center» of the Healthcare Ministry. Saint-Petersburg, Russia
The target audience of this peer-reviewed journal is cardiologists and internal disease specialists. The journal is primarily focused on original studies, cardiac surgery, and cardiac pharmacotherapy. It also publishes lectures and literature reviews on various problems of modern cardiology, reports on new diagnostic methods, and other information which is important for the practitioners. The aim of the journal is both scientific and practical, also with referring to organizing matters of the RSC. The best of all cardiological research in Russia is submitted to Journal.
The language of publication is Russian, with contents and abstracts of all the articles presented in English. The Journal also accepts manuscripts from foreign authors and publishers them in English with abstracts in Russian.
Science Index (2023) 9,294 (5th procentile, 9 in "Medicine and healthcare")
Impact-factor (2023) 1,799
Current issue
ARTERIAL HYPERTENSION
- Patients with uncontrolled resistant hypertension have more pronounced thoracic aortic calcification compared to patients who have achieved the target blood pressure level.
- The calcium score correlates with individual parameters of 24-hour blood pressure monitoring, which may indicate the contribution of thoracic aortic calcification to resistant hypertension progression.
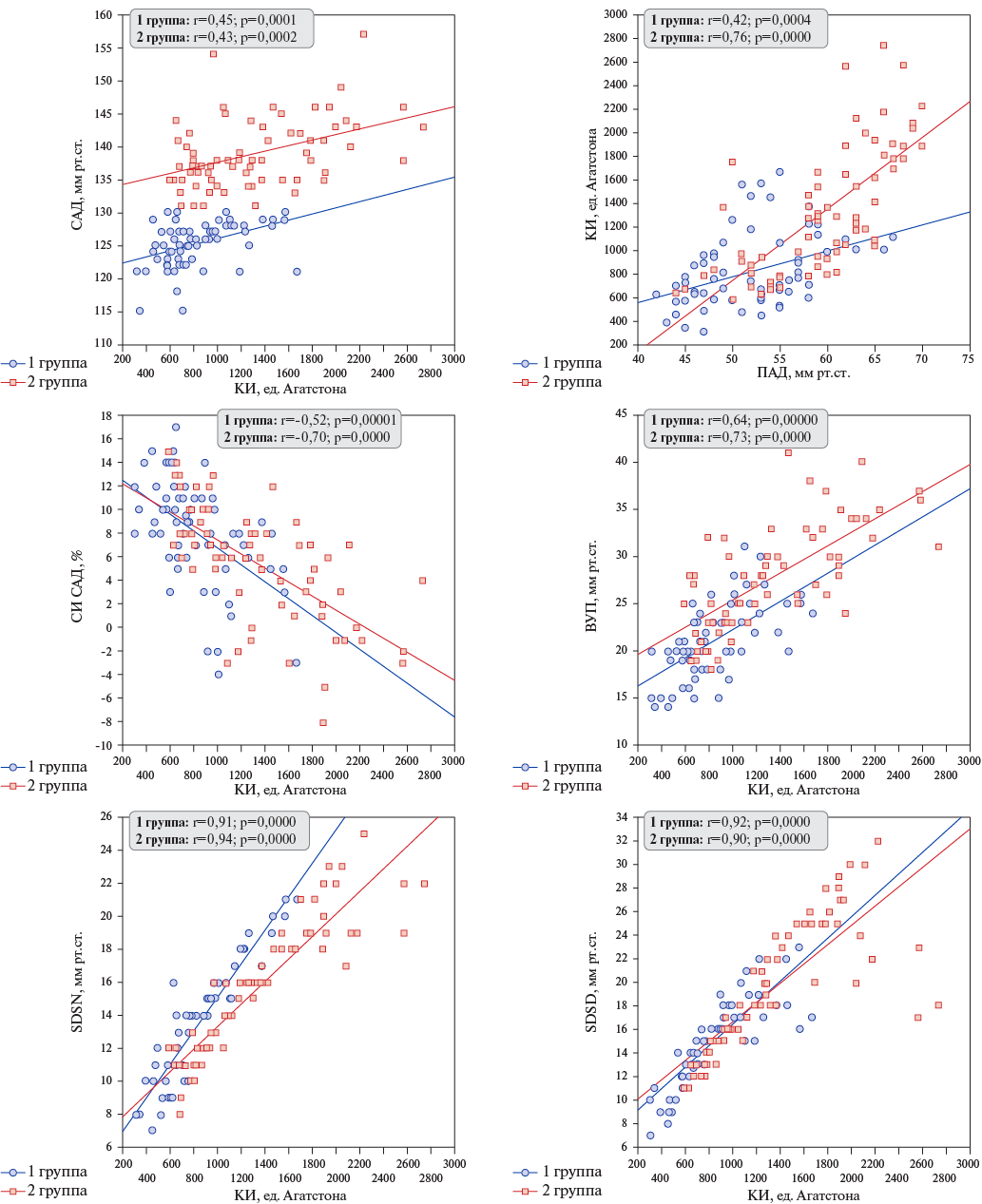
Aim. To evaluate thoracic aortic calcification and parameters of 24-hour ambulatory blood pressure monitoring (ABPM) in patients with resistant hypertension (HTN).
Material and methods. The study included 138 patients diagnosed with resistant HTN. Based on ABPM (Schiller BR-102 plus), the patients were divided into groups of controlled (Group 1, n=68) and uncontrolled resistant HTN (Group 2, n=70). Thoracic aortic calcium score was determined using a 64-slice computed tomography system (Siemens, Germany).
Results. No significant differences were found between the groups in the key clinical and anthropometric characteristics. The Agatston calcium score ranged from 312 to 2738 and was higher in the group of uncontrolled HTN (p<0,00001). ROC analysis found that calcium score of 900 with a sensitivity of 71,4% and a specificity of 66,2% differentiates individuals with controlled and uncontrolled resistant HTN (AUC=0,791). According to ABPM, the most significant differences were obtained when comparing pulse pressure, 24-hour systolic blood pressure (BP) index, morning surge, and daytime systolic BP variability. Regardless of the effectiveness of antihypertensive therapy, the calcium score correlated positively with the variability of systolic BP, pulse BP, and morning surge, and negatively with the 24-hour systolic BP index, but the relationship strength was greater when the target BP was not reached.
Conclusion. In patients with resistant HTN without BP control, higher values of pulse pressure, morning surge, and systolic BP variability, and a decrease in the 24-hour systolic BP index were noted. The calcium index was higher in the group of patients with uncontrolled resistant HTN and was associated with the variability of systolic BP, pulse pressure, morning surge, and nocturnal systolic BP decrease.
- The study confirms the long-term effectiveness of renal denervation, showing a significant decrease in mean 24-hour systolic blood pressure over 5 years without accelerating the renal function decline rate, as well as left ventricular myocardial structural improvement.
- The work was the first to establish predictors of renal denervation effectiveness, including, in addition to the initial level of mean 24-hour systolic blood pressure, its variability and the level of kaliuresis, which may help in individualizing the selection of patients for this expensive procedure.
Aim. To evaluate the long-term effectiveness of renal denervation (RDN) in reducing blood pressure (BP) and cardio- and nephroprotection in patients with resistant hypertension based on five-year follow-up.
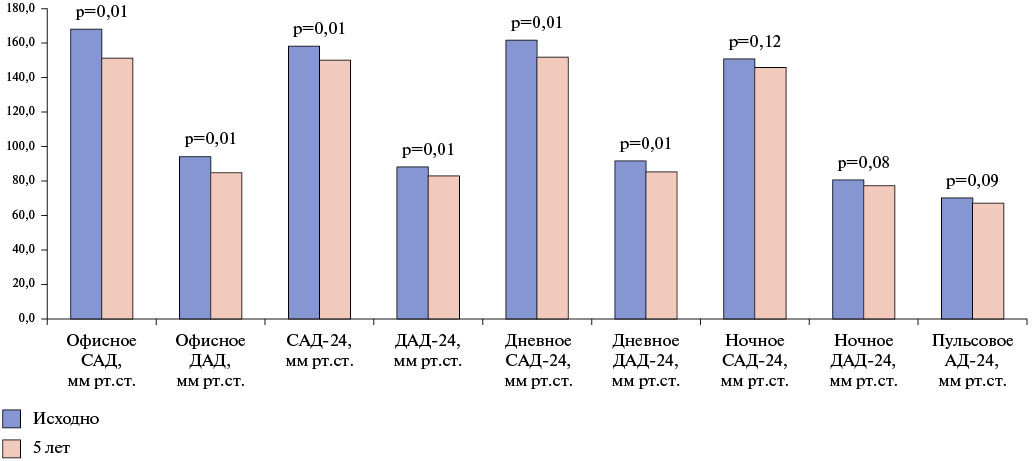
Material and methods. A total of 53 patients who completed a five-year follow-up period after RDN were examined (mean age 56,3±9,2 years, 23 men (43%), mean 24-hour BP (BP-24) — 168/94 mm Hg). Office and mean 24-hour BP were assessed. Left ventricular mass (LVM) were measured using echocardiography data. Renal function was evaluated using the estimated glomerular filtration rate (eGFR) (CKD-EPI), 24-hour urine volume, 24-hour urine protein and albumin excretion, daily K- and Na-cut. The primary endpoint of RDN efficacy was considered to be a decrease in systolic BP (SBP)-24. There were following secondary endpoints: achievement of target BP, proportion of responders (individuals with decrease in SBP-24 by 5 mm Hg or more), decrease in LVM, slowing of eGFR decline rate (change in eGFR <3 ml/min/1,73 m2 per year).
Results. Five years after RDN, significant SBP-24 decrease was registered on average in the group (p=0,01). Target clinical SBP was achieved by 15 patients (28,3%). There were 28 responders (52,8%).
According to echocardiography, significant decrease in interventricular septal thickness was noted (p=0,01) in the absence of significant decrease in LVM (p=0,2). Annual decline rate in eGFR was 2,56 ml/min/1,73 m2. An increase in 24-hore urine volume (p=0,02) and sodium excretion (p=0,01) was documented. The degree of reduction in SBP-24 had a direct quantitative relationship with the increase in 24-hour natriuresis (r=-0,63; p=0,017). According to the ROC analysis, the predictors of response to RDN were the initial level of SBP-24 (>155,5 mm Hg), variability of SBP-24 (>5,5 mm Hg) and kaliuresis level (>27,2 mmol/l).
Conclusion. RDN in patients with resistant HTN is accompanied by a stable 5-year antihypertensive effect without accelerating the renal function decline rate, as well as myocardial structural improvement in the form of a decrease in interventricular septal thickness. One of the pathophysiological mechanisms for BP reduction may be an increase in natriuresis, and its predictors are the initial levels of SBP-24, its variability, and 24-hour kaliuresis.
- Detection of elevated central hemodynamics and aortic vascular stiffness in masked hypertension (HTN) in overweight/obese women aged 18 to 35 indicates a possible aortic damage as a target organ, despite initial office normotension and young age.
- A decrease in the peripheral augmentation index in the discussed contingent for all HTN phenotypes and its negative correlation with anthropometric indicators confirms physiological adaptive reaction at the indicated age from smaller arteries in response to body weight increase. Such a reaction is most pronounced in masked hypertension.
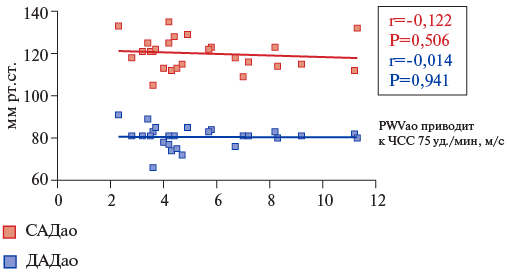
Aim. To evaluate central hemodynamics and vascular stiffness (VS) from the perspective of hypertension (HTN) phenotype in overweight/obese young women.
Material and methods. A total of 104 women with overweight and obesity, aged 18 to 35 years (28,41±0,46), were examined. Based on office and outpatient blood pressure measurements, four following groups were formed: group 1 — persistent normotension (control); group 2 — white coat HTN; group 3 — masked HTN; group 4 — persistent HTN. We studied risk factors, features of central aortic pressure and HF. We used the BPLab diagnostic system (Petr Telegin, Russia). A correlation analysis was performed between HF indicators and some risk factors of the examined subjects.
Results. In the examined women with masked and persistent HTN, the greatest differences from the control group were noted in the 24-hour central hemodynamics parameters — systolic aortic pressure, diastolic aortic pressure, mean aortic pressure and pulse aortic pressure. When assessing aortic stiffness in the specified group of individuals, the maximum RWVao/RWV values reduced to the heart rate of 75 bpm were found in groups with masked and persistent HTN, which significantly exceeds their values in the control group (Р1-3=0,0002, Р1-4<0,0001; Р1-3=0,0111, Р1-4=0,0125, respectively). Similar changes were noted in the aortic augmentation index. Correlation analysis revealed significant positive relationship between the VS and BMI, as well as waist circumference.
Conclusion. In overweight and obese young women with masked phenotype of HTN, reliably high values of central hemodynamic parameters were found relative to normotensive women. Signs of arterial wall remodeling have been established not only in persistent but also in masked HTN. These data should be taken into account when examining the specified group of individuals and developing measures aimed at identifying masked HTN due to its proven contribution to the development of cardiovascular disease.
ИНФАРКТ МИОКАРДА
- In patients with severe course of coronavirus disease 2019 (COVID-19), the troponin level increases regardless of the presence of acute coronary syndrome (ACS).
- In patients with COVID-19 with ACS, depending on variant (unstable angina and myocardial infarction (MI)) the most informative parameters were established (SAPS II and interleukin (IL)-1β). To predict the outcome of ACS, a logistic model with a sensitivity of 97% and a specificity of 97% was created.
- In patients with COVID-19 complicated by MI, when specifying variant (with and without ST-segment elevation), the SOFA score and IL-6 were of primary importance, while the model for predicting MI variants had a sensitivity of 91% and a specificity of 85%.
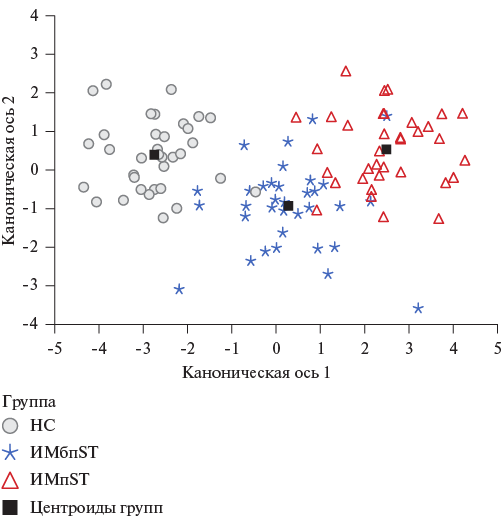
Aim. Based on the study of individual biomarkers in patients with a coronavirus disease 2019 (COVID-19) in combination with acute coronary syndrome (ACS), to develop a method for predicting the course type.
Material and methods. The study included patients with severe COVID-19 and ACS (n=104) of three variants: subgroup 1 (n=35) — unstable angina (UA); subgroup 2 (n=34) — non-ST-elevation myocardial infarction (NSTEMI); subgroup 3 (n=35) — ST-elevation MI (STEMI).
Results. In patients with COVID-19 and ACS, the following was observed: a significant lung damage according to computed tomography (%) — 45,00 (35,00; 55,00), high scores on intensive care severity scales: SOFA — 16,00 (14,00; 18,00) and SAPS II — 21,00 (17,00; 24,00), as well as elevated values of C-reactive protein (mg/l) — 129,60 (74,55; 198,68), creatine phosphokinase (CPK) (U/l) — 1986,50 (1204,50; 2163,00), lactate dehydrogenase (U/l) — 1117,50 (711,25; 1458,00), troponin (ng/l) — 82,50 (63,00; 119,50) and ferritin (ng/lm) — 965,50 (757,25; 1222,50). Among the cytokine profile parameters, both increased (interleukin (IL)-1β (pg/ml) — 8,94 (8,48; 9,50)) and decreased (IL-4 (pg/ml) — 10,52 (10,01; 10,91); IL-10 (pg/ml) — 85,11 (83,02; 87,98); interferon-γ (pg/ml) — 9,27 (8,58; 9,85)) values were recorded. In the subgroup with STEMI, the highest SOFA (Me=18,00; p1-3=0,003 and p2-3<0,001) and SAPS II (Me=25,00; all p<0,001) scores were found. In patients with UA, the blood total protein content was higher (p1-2<0,001 and p1-3=0,003), and the level of C-reactive protein and CPK was lower (p<0,001 for all) than in the comparison subgroups. In addition, these patients had highest values of IL-4 (Me=10,91 pg/m; p<0,001), IL-10 (Me=86,60; p=0,002), interferon-γ (Me=9,75; pg/ml, p1-2=0,002 and p1-3<0,001) and the lowest levels of IL-1β (Me=8,51 pg/ml; p<0,001), IL-6 (Me=14,90 pg/ml; p<0,001), tumor necrosis factor-α (Me=22,21 pg/ml, p1-3=0,009).
Conclusion. The main contribution to divided prediction of UA and MI was made by the SAPS II score and IL-1β, and to a lesser extent by CPK and IL-6. To clarify the MI variant (with and without ST-segment elevation) — the SOFA scale and IL-6 contribution was significant. The obtained discriminant models have a sensitivity of 97% and 91%, and a specificity of 97% and 85%, respectively.
- The proven role of HIV infection in atherogenesis and the continuing increase in the number of HIV-positive people leads to an increase in their proportion among patients with myocardial infarction (MI) in the general population.
- It is necessary to generalize the experience and obtain new data on the problem of MI in HIV-infected patients.
- The work establishes the clinical features of MI in HIV infection in the Russian population of patients hospitalized in regional vascular centers as follows: a younger age of patients, predominantly anterior MI and left anterior descending artery involvement, more frequent left ventricular systolic dysfunction, as well as comorbidity with anemia.
Aim. To compare the clinical characteristics of acute myocardial infarction (MI) in HIV-infected patients hospitalized in regional vascular centers.
Material and methods. This retrospective analysis included 5990 medical records of patients with MI, among which a group of 38 HIV-infected patients was identified. The control group of patients with MI without HIV infection (n=114) was formed randomly. The groups were compared for demographic data, cardiovascular risk factors (RF), clinical and paraclinical parameters characterizing MI. Associations of MI characteristics with HIV status were assessed using univariate and multivariate logistic regression adjusted for sex, age, body weight and cardiovascular RFs.
Results. Patients with HIV infection, in contrast to HIV-negative patients, were younger (median age 47 and 63 years, respectively). They had a lower body mass index (23,9 and 27,7 kg/m2), lower blood levels of total cholesterol (4,6 and 5,1 mmol/L), non-high-density lipoprotein cholesterol (3,4 and 3,9 mmol/L), glucose (5,8 and 7,1 mmol/L), high-sensitivity C-reactive protein (hsCRP) (5,6 and 24,9 mg/L) and hemoglobin (139,5 and 149,0 g/L), and higher levels of cardiac troponin I (8,0 and 4,1 pg/ml). In the HIV group, anterior MI (71,1% and 41,2%), left anterior descending artery (LAD) involvement (70,4% and 43,0%), left ventricular (LV) systolic dysfunction (36,8% and 20,2%), anemia (34,2% and 7,1%) were more common, while obesity (7,9% and 31,6%) and three-vessel disease (6,9% and 36,0%) were less common. HIV-positive patients underwent coronary angioplasty less often (68,4% and 93,9%). In the adjusted multivariable regression model, independent associations of HIV infection with anterior MI (odds ratio [95% confidence interval] 3,06 [1,05-8,88]), LAD involement (3,5 [1,09-11,29]), three-vessel disease (0,17 [0,03-0,92]), LV systolic dysfunction (4,55 [1,37-15,13]), anemia (8,51 [1,73-41,94]), and hsCRP >5 mg/L (0,08 [0,01-0,49]) were found.
Conclusion. In HIV-infected patients with MI treated in a regional vascular center, anterior MI, LAD disease, LV systolic dysfunction, anemia were more common, blood hsCRP levels were lower, and three-vessel disease was detected less often. Moreover, HIV-infected patients were younger and had fewer traditional cardiovascular risk factors, which suggests additional HIV-associated mechanisms of MI development.
- Myocardial infarction (MI) in patients with chronic kidney disease (CKD) is characterized by a more severe course and a higher number of complications than in patients with normal renal function.
- Patients with MI and CKD are less likely to undergo coronary angiography and percutaneous coronary intervention, and they often do not receive drug therapy in full.
- Mortality in patients with MI and CKD is significantly higher compared to mortality in patients with preserved renal function both at the hospital stage and one year after the index event.
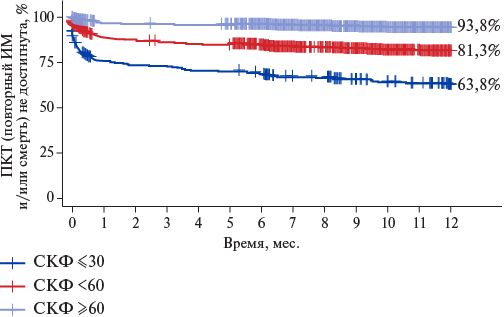
Aim. To evaluate the prognosis of patients with myocardial infarction (MI) and chronic kidney disease (CKD) based on the data of the Russian registry REGION-MI, as well as to clarify the disease course and treatment of this group of patients in real-world practice.
Material and methods. REGION-MI is a Russian multicenter prospective observational study that included 10884 patients with acute MI. Data on creatinine levels and glomerular filtration rate (GFR) were obtained from 10229 people.
Results. Among patients included in the REGION-MI registry, a decrease in GFR <60 ml/min/1,73 m2 was diagnosed in 30,5%. Patients with MI and CKD are significantly older than patients with preserved renal function, have a greater number of comorbidities. In addition, they were more often diagnosed with non-ST-elevation MI and were less likely to undergo coronary angiography and percutaneous coronary intervention. Patients with CKD were less likely to receive all groups of drugs prescribed after MI. Mortality of patients with CKD in our study was significantly higher compared to mortality of patients with preserved renal function both at the hospital stage (8,4% and 1,7%, respectively, odds ratio 5,31; 95% confidence interval: 4,25-6,62; p<0,005) and one year after the index event (10,1% and 3,6%, respectively, odds ratio 3,03; 95% confidence interval: 2,54-3,61, p<0,005).
Conclusion. A decrease in GFR is a factor influencing an increase in mortality in MI patients. Patients with CKD and MI have a very high risk of cardiovascular events, as well as require intensive care in the acute and late periods of the disease. However, they often do not receive drug therapy in full and are less likely to undergo coronary angiography and invasive treatment. Large clinical trials are needed to study the characteristics of the disease course and choose the optimal treatment tactics for patients with MI and reduced renal function.
ИШЕМИЧЕСКАЯ БОЛЕЗНЬ СЕРДЦА
- Regional changes of hospitalization rate of patients for chronic coronary artery disease (CAD) in Russia as a whole and its regions in 2014-2023 vary significantly.
- For correct comparisons of indicators in dynamics, changes in approaches to collecting statistical information are necessary.
- Due to the large number of factors influencing the hospitalizations for chronic CAD, influence of each of them in the context of practical healthcare in Russia should be assessed.
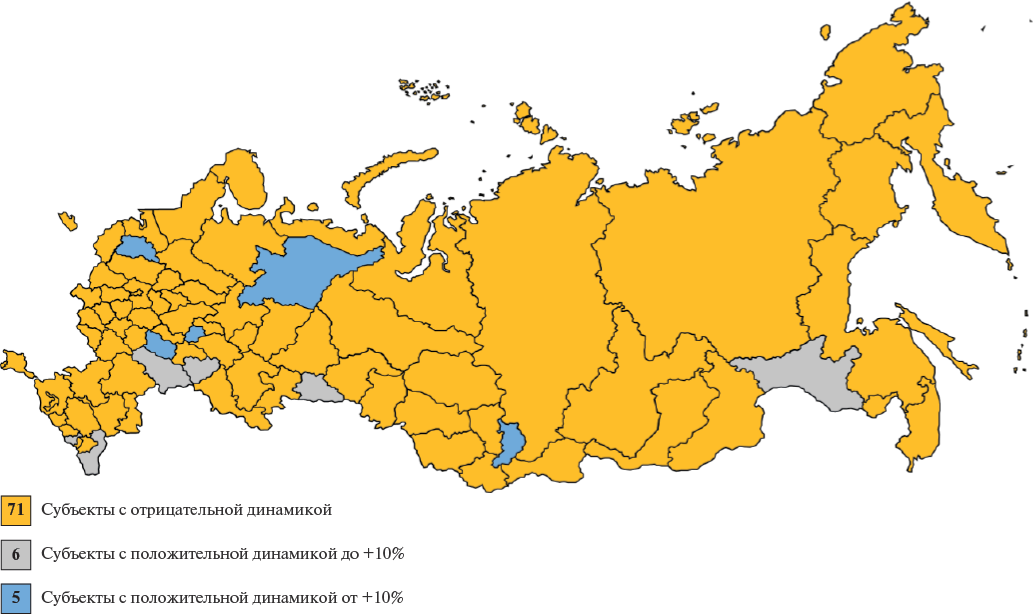
Aim. To assess the changes and variability of hospitalization of patients for chronic coronary artery disease (CAD) in the Russian Federation and its subjects in 2014-2023.
Material and methods. We analyzed Rosstat data on the hospitalization structure for CAD/chronic CAD/old myocardial infarction (MI) among adults (18 years and older), contained in table 2000 of the federal statistical observation form № 14 and assessed its changes for 2014-2023. The average regional rates of hospitalization with CAD/chronic CAD/old MI per 100 thousand of the adult population (M±σ), relative values (%) were determined. SPSS 26.0 (IBM Company) and Excel (Microsoft for Microsoft Windows) packages were used for statistical analysis.
Results. The mean regional hospitalization rate of patients due to CAD in 2014 was 1612,0±416,8 per 100 thousand of the adult population, in 2023-1331,8±448,4 per 100 thousand of the adult population (p<0,0001; visibility index 82,7±15%). The mean regional hospitalization rate of patients due to chronic CAD in 2014 was 550,9±325,7 per 100 thousand of the adult population, in 2023-551,4±367,5 per 100 thousand of the adult population (p=0,9; visibility index 107,3±47,4%). The mean regional share of hospitalization due to chronic CAD in the overall hospitalization structure due to CAD in 2014 was 33,4±15,7%, in 2023-39,4±16,2%. The coefficient of variation in hospitalization rate due to CAD increased from 25,8% to 33,7%; due to chronic CAD — from 59,5% to 66,6%. In 2023, compared to 2014, a significant (p<0,0001) increase in old MI contribution to hospitalization rate due to chronic CAD was noted as follows: the mean regional value in 2014 was 25,1±16,7%, and in 2023-32,4±19,3%. In 36 regions, a decrease in the relative and absolute number of hospitalizations of patients due to both CAD and chronic CAD was recorded; in 7 regions, an increase was recorded, while in 39 regions, there were multidirectional changes.
Conclusion. Regional changes in hospitalization rate due to chronic CAD and the contribution of chronic CAD to CAD in Russia as a whole and Russian regions in 2014-2023 vary significantly. No unidirectional changes were noted over a 10-year period. Correct comparison of the indicators over time requires changes in approaches to collecting statistical information. The identified trends may be associated with both approaches to organizing treatment and diagnostic care and the specifics of recording the reasons for hospitalization according to ICD-10 codes. Due to the large number of factors influencing the hospitalizations for chronic CAD, influence of each of them in the context of practical healthcare in Russia should be assessed.
ACUTE AND CHRONIC HEART FAILURE
- Frailty syndrome is common among hospitalized patients with heart failure, making a comprehensive assessment of geriatric status in this cohort of patients important.
- Patients with heart failure and concomitant frailty were characterized by a severe functional class, prolonged intravenous diuretic therapy, frequent association with cognitive and functional impairment, and poor prognosis.
- Given the potential reversibility of frailty, heart failure therapy optimization and a comprehensive assessment of geriatric patients are particularly important to improve the prognosis of both diseases.
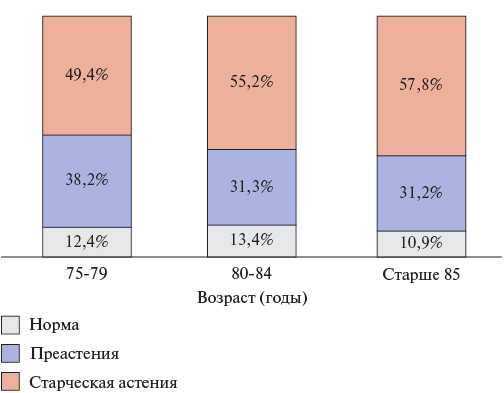
Aim. To study the prevalence of frailty syndrome and major geriatric syndromes in hospitalized patients with heart failure (HF), as well as the prognosis depending on frailty severity.
Material and methods. We prospectively included 250 patients over 75 years old, hospitalized for decompensated HF (median age, 83,0 [77,0-86,0] years; men, 41,6% (n=104)). In addition to traditional paraclinical investigations, including N-terminal pro-brain natriuretic peptide and echocardiography, all patients were assessed for frailty using the "Age Is Not a Barrier" questionnaire on the 5th day of hospitalization. Score of 2 or less was recognized as absence of frailty, while score of 3-4 — as probable prefrailty, and score of 5-7 — probable frailty. Patients with intermediate score of 3-4 were given a brief physical functioning tests to clarify the frailty. To assess the prevalence of other geriatric syndromes, all patients underwent cognitive function assessment using the Montreal Cognitive Assessment and functional independence using the Barthel scale. The primary endpoint was all-cause inhospital mortality.
Results. The prevalence of SSA was 64,0% (n=160) in hospitalized patients with HF. The frequency of preserved left ventricular ejection fraction in patients with HF and frailty was 51,1%. Patients with frailty and HF were characterized by worse exercise tolerance (NYHA class III-IV, 90,6% vs. 65,6%, p<0,05), higher N-terminal probrain natriuretic peptide (2912,5 [1709,0-6455,0] vs. 1903,1 [1577,3-3031,8] pg/ml, p<0,05) compared to patients with HF and without frailty. The duration of intravenous diuretic therapy and hospitalization in patients with frailty and HF were higher than in patients without frailty (7,1±3,4 vs. 5,5±3,4 days (p<0,05); 8,1±3,5 vs. 7,1±2,7 days (p<0,05), respectively). The primary endpoint was achieved in 16,1% (n=22) with concomitant frailty compared to 7,1% (n=8) in patients with HF and without frailty (p<0,05). Frailty increased the probability of inhospital mortality by almost 3 times in elderly patients with HF (OR 2,8; 95% CI 1,2-6,4, p<0,05).
Conclusion. The relevance of a comprehensive geriatric assessment in an elderly patient with HF is due to the high prevalence of frailty in this cohort of patients and its significant impact on the prognosis. Identification of frailty can help in making important clinical decisions, identifying a high-risk group for complications, and possibly optimizing treatment. Given that frailty can be potentially reversible, this particularly emphasizes the importance of optimizing HF therapy, on the one hand, and conducting a comprehensive frailty assessment in elderly patients with HF, on the other, to improve the prognosis of both diseases.
What is already known about the subject?
- The group of patients with heart failure with preserved ejection fraction is characterized by pronounced heterogeneity and multimorbidity.
- High medication adherence in patients with heart failure is associated with a lower hospitalization rate and a better disease course.
What might this study add?
- Patients who visit the doctor more often and have a high level of awareness of current glucose and cholesterol levels have a higher level of treatment adherence.
- Patients without a history of coronary artery disease or myocardial infarction have lower adherence to drug therapy, reflecting the need for increased attention to measures to improve their adherence to treatment in the outpatient setting.
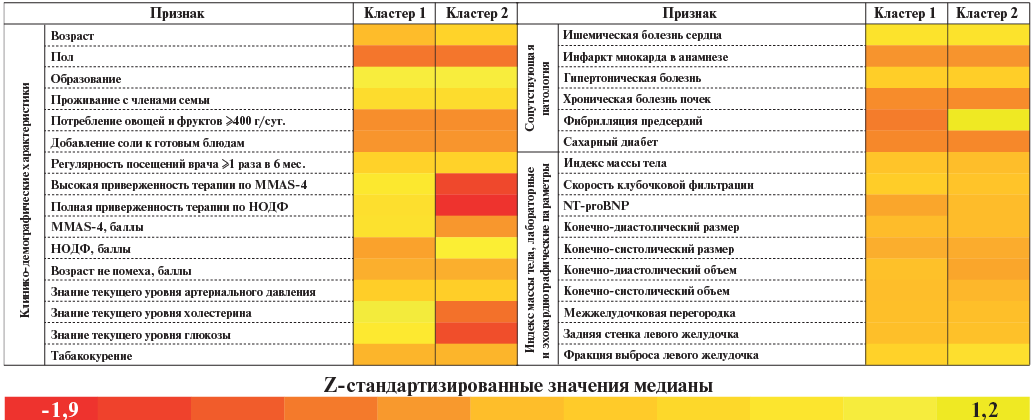
Aim. To identify phenotypes of patients with heart failure with preserved ejection fraction (HFpEF) aged 60 years and older using cluster analysis based on clinical characteristics and treatment adherence level.
Material and methods. The observational study included 212 outpatients aged ≥60 years diagnosed with HFpEF. Adherence was determined using the Morisky Medication Adherence Scale-4 (MMAS-4) and the National Society for Evidence-Based Pharmacotherapy (NSEPh) adherence scale for patients with noncommunicable diseases. Probable frailty was assessed using the "Age Is Not a Barrier" questionnaire. To identify phenotypes, a cluster analysis was performed using the Ward method with z-scores.
Results. The median MMAS-4 score was 4 [3; 4], while high adherence was recorded in 68,9% of patients. The median NSEPh adherence was 0 [0; 0], while full adherence was recorded in 78,3% of patients. The median "Age Is Not a Barrier" questionnaire score was 1 [0; 3]. No significant relationships between the studied parameters were revealed during the correlation and regression analysis. The optimal number of clusters was 2 as follows: 163 (76,9%) patients in cluster 1, 49 (23,1%) in cluster 2. Patients in group 1 had higher adherence to therapy (p<0,001), visited a doctor more often (p<0,001), and more often had a history of coronary artery disease (p=0,032) and myocardial infarction (p=0,006). Patients in group 2 were older (p=0,016), had a higher risk of probable frailty (p=0,021) and were less informed about current blood glucose (p<0,001) and cholesterol (p=0,001) levels. The groups did not differ significantly in the frequency of drug prescriptions.
Conclusion. High adherence is associated with frequent visits to the doctor and high patient awareness. Patients with non-ischemic HFpEF require additional monitoring and measures to improve treatment adherence.
PROGNOSIS AND DIAGNOSTICS
- Norepinephrine, adrenomedullin and catestatin levels did not differ significantly between patients with or without coronary microvascular dysfunction (CMD).
- Cathestatin concentrations were significantly correlated with resting myocardial flow and heart rate variability parameters. Serum norepinephrine levels were associated with myocardial flow reserve, while adrenomedullin levels — with mean NN.
- The only independent factors associated with CMD were rMSSD ≤60 ms and body mass index ≥27,8 kg/m2.
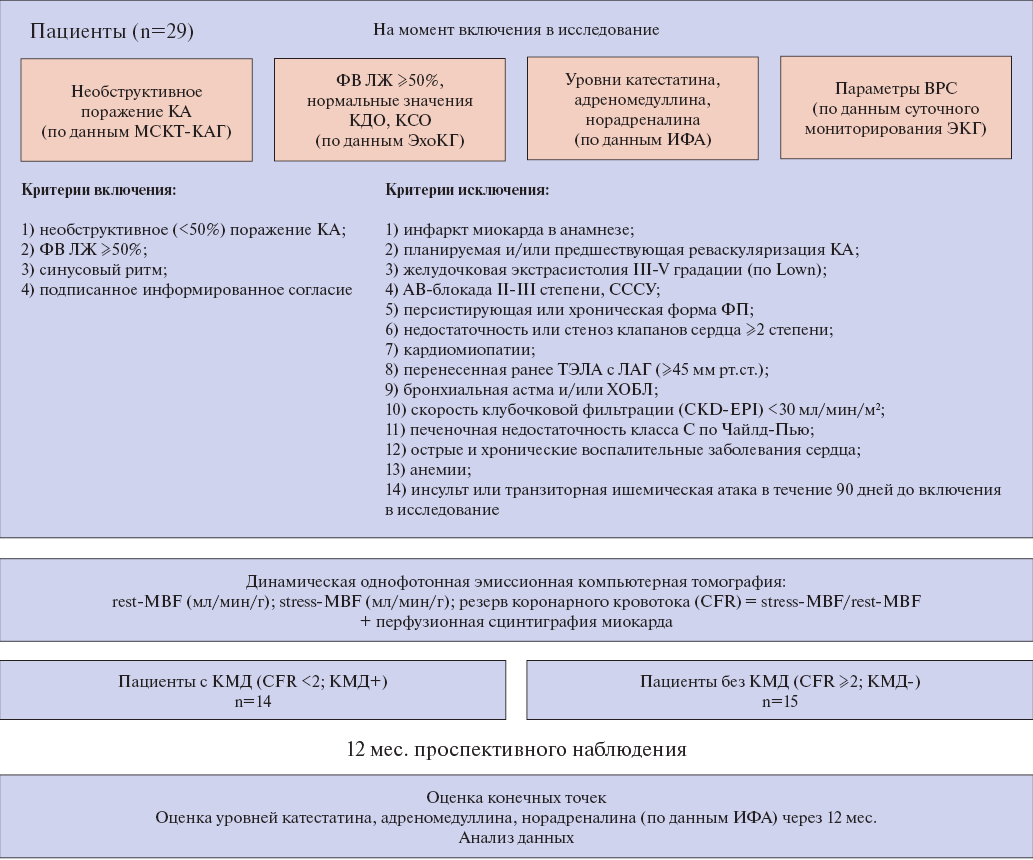
Aim. To study the relationship between adrenomedullin, catestatin, norepinephrine and heart rate variability (HRV) parameters with coronary microvascular dysfunction (CMD) in patients with non-obstructive coronary artery disease (CAD).
Material and methods. The study included 29 patients (55 (51; 63) years) with preserved left ventricular ejection fraction (63 (61; 66)%) and non-obstructive CAD. Serum biomarker levels were assessed at baseline and after 12-month follow-up using enzyme immunoassay. Standard semiquantitative scores of myocardial perfusion impairment and myocardial flow parameters were assessed using dynamic single-photon emission computed tomography. In the absence of obstructive CAD, a decrease in myocardial flow reserve (MFR) ≤2 was regarded as CMD. HRV indices were determined using 24-hour ECG monitoring.
Results. Depending on CMD, patients were divided into 2 following groups: CMD+ (n=14) and CMD- (n=15). According to 24-hour ECG monitoring, patients with CMD showed a decrease in HRV and sympathetic activity. Cathestatin levels significantly correlated with myocardial flow at rest (r=0,329; p=0,019) and HRV parameters as follows: mean duration of all R-R (N-N) intervals of sinus rhythm (mean NN) (r=-0,410; p=0,001), SDANN (r=-0,276; p=0,036) and SDNNidx (r=0,287; p=0,029). Norepinephrine concentrations were interrelated only with CFR (r=-0,295; p=0,037), and adrenomedullin — with mean NN (r=0,272; p=0,038). Biomarker levels did not differ significantly between the groups at baseline and after 12 months. At the same time, norepinephrine levels remained virtually unchanged during prospective follow-up, while catestatin levels in CMD+ patients tended to increase by 11,7% (p=0,632), and in the CMD- group — by 16,1% (p=0,632), and adrenomedullin — by 19,4% (p=0,325) and 23,7% (p=0,527), respectively. Independent factors associated with CMD were sympathetic suppression, expressed as a decrease in square root of the mean squared differences of successive NN intervals (rMSSD) ≤60 ms (odds ratio 1,065; 95% confidence interval 1,005-1,675; p=0,001) and body mass index ≥27,8 kg/m2 (odds ratio 1,061; 95% confidence interval 0,998-1,668; p=0,001).
Conclusion. Norepinephrine, adrenomedullin, and catestatin levels did not differ significantly between patients with and without CMD. However, catestatin concentrations were associated with resting myocardial flow and HRV parameters, while norepinephrine values — with CFR, and adrenomedullin — with mean NN.
- The problem of verification of chronic myocarditis in patients with atrial fibrillation of unknown origin is considered, which is associated with diagnostic limitations of the magnetic resonance imaging (MRI) and the limited use of endomyocardial biopsy in clinical practice.
- The study showed that edema according to cardiac MRI data is the only sign that has predictive value for the severity of inflammatory cell infiltration in myocardial fragments according to histological examination.
- The combined use of contrast-enhanced cardiac MRI and endomyocardial biopsy improves the diagnosis of chronic myocarditis in patients with atrial fibrillation of unknown origin.
Aim. To analyze the significance of contrast-enhanced cardiac magnetic resonance imaging (MRI) and endomyocardial biopsy (EMB) in the diagnosis of myocarditis in patients with atrial fibrillation (AF) of unknown origin.
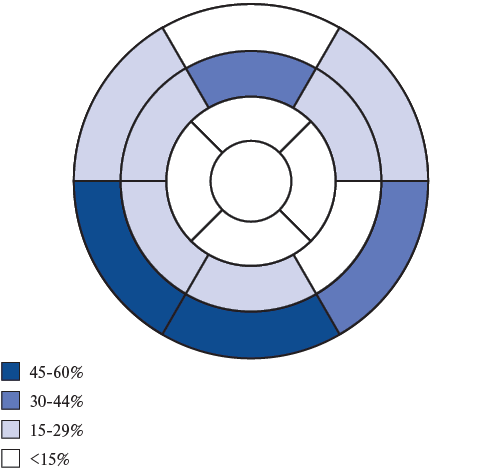
Material and methods. The study included 57 patients with AF of unknown origin aged 45,5 [38,8;53,3] years (men, 77,2%). Paroxysmal AF was observed in 56,1% of patients, while persistent AF — in 22,8%, and long-standing persistent AF — in 21,1%. Thirty-five patients underwent contrast-enhanced cardiac MRI and Lake-Louise criteria assessment. Simultaneously with AF ablation, all patients underwent EMB from the interventricular septum, outflow tract, and right ventricular apex with histological diagnosis of myocarditis based on the Dallas criteria modified by the World Heart Federation.
Results. According to contrast-enhanced cardiac MRI, delayed contrast accumulation was diagnosed in 91,4%. In 17,1% of cases, signs of edema were detected on T2-weighted images, while the average left ventricular (LV) edema level was 1,6±0,3 (reference <2,0). In 25,7% of patients, signs of hyperemia were detected with average LV hyperemia index of 3,4 [2,2;4,0] (reference <4,0). Myocarditis was diagnosed in 12 patients (34,3%) with 3 criteria detected in 2 patients, 2 in 10 patients (6 with hyperemia + fibrosis, 4 with edema + fibrosis), and 1 (fibrosis) in 22 patients. Histological criteria of lymphocytic myocarditis were detected in 28 out of 57 patients (49,1%): focal in 19 (67,9%), diffuse in 6 (21,4%), and diffuse-focal in 3 (10,7%). Edema signs on MRI was the factor most strongly associated with the total number of detected T-lymphocytes in myocardial fragments, assessed using ROC analysis (AUC 0,782 (95% confidence interval 0,61-0,93) p=0,032). The combined use of MRI and EMB allowed to increase the accuracy of myocarditis diagnosis from 34,3 to 62,9%.
Conclusion. Myocarditis was diagnosed in 34,3% of patients according to MRI and in 49,1% according to EMB. Edema according to MRI data was the only sign that had predictive value for the severity of inflammatory cell infiltration in myocardial fragments. Histological analysis in combination with MRI increased the accuracy of myocarditis diagnosis in patients with AF of unknown origin from 34,3 to 62,9%.
- Circulating biomarker profile reflects structural changes in patients with hypertrophic cardiomyopathy.
- The association of circulating fibrosis biomarkers with the myocardial expression of relevant genes in patients with hypertrophic cardiomyopathy was confirmed.
- Long-term prognosis after septal reduction may be determined by the severity of myocardial fibrosis.
Aim. To compare the profile of circulating biomarkers and expression of relevant fibrosis genes in the myocardium with clinical and morphological data on the severity of myocardial fibrosis in patients with obstructive hypertrophic cardiomyopathy (HCM) who underwent septal myectomy.
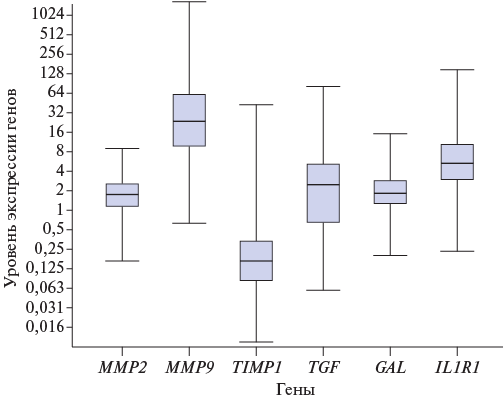
Materials and methods. This prospective study included 69 patients with obstructive HCM and indications for septal reduction. The results of paraclinical investigation, echocardiography, cardiac magnetic resonance imaging, histological examination, serum biomarker levels (transforming growth factor beta-1 (TGF-β1), matrix metalloproteinase-9 (MMP-9), tissue inhibitor of matrix metalloproteinases-1 (TIMP-1), galectin-3, soluble interleukin-1 receptor 4 (ST2) (sST2), C-telopeptide of type I collagen (CITP), C-terminal propeptide of type I collagen (PICP) and N-terminal propeptide of type III procollagen (PIIINP)), analysis of RNA obtained from intraoperative myocardial biopsies were assessed.
Results. Increased serum levels of galectin-3, TGF-β1, sST2 and collagen synthesis markers, as well as the level of the collagen degradation marker CITP were revealed. Relationships were established between the PIIINP level and interventricular septum thickness indexed to the body surface area (p=0,049), as well as the left atrial diameter (p=0,024). An increase in the expression levels of relevant fibrosis genes, with the exception of TIMP1, was noted. An increased level of circulating PIСP was associated with an increase in the expression of galectin-3 and interleukin-1 receptor type 1 genes in the myocardium. Septal myectomy allowed revealing that patients without improvement in N-terminal pro-brain natriuretic peptide had a higher sST2 level. A negative relationship was established between the MMP9 gene expression in the myocardium and changes of the left atrial size in the long-term period after septal myectomy (p=0,032).
Conclusion. The profile of circulating biomarkers is associated with the expression of relevant fibrosis genes in the myocardium and is a promising non-invasive method for assessing the activity of fibrosis processes. Myocardial fibrosis plays an important role in assessing the prognosis during the follow-up of patients with HCM.
CLINIC AND PHARMACOTHERAPY
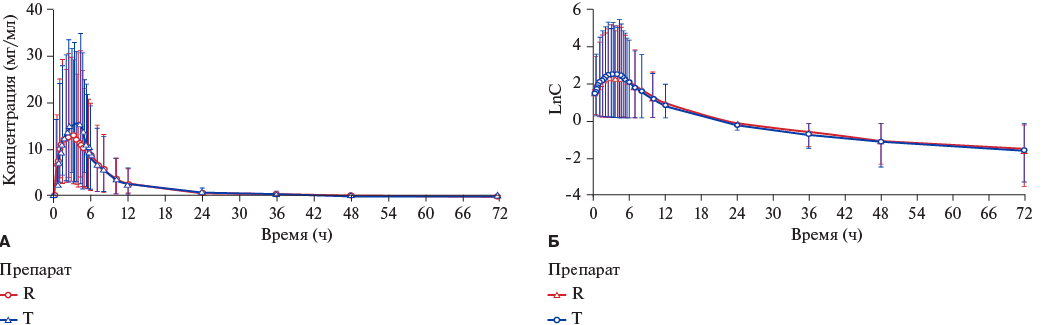
Aim. To assess comparative pharmacokinetics and establish bioequivalence of film-coated Rosuvastatin 20 mg (OOO NTFF "POLYSAN", Russia) (T) and film-coated Crestor® 20 mg (AstraZeneca UK Limited, UK) (R) after a single dose of 20 mg on an empty stomach in healthy volunteers, as well as to study their safety and tolerability.
Material and methods. This open-label, randomized, crossover, two-period study of comparative pharmacokinetics and bioequivalence of T and R following a single dose in the fasted state was conducted in 46 healthy volunteers at a single center. After randomization, volunteers in each Study Period received a single 20 mg rosuvastatin dose in a different sequence (TR or RT). Periods I and II were separated by a 14-day washout period. Plasma rosuvastatin concentrations were determined by high-liquid chromatography–mass spectrometry. Following pharmacokinetic parameters were calculated: area under the concentration-time from 0 to 72 h (AUC0-t) and the maximum concentration (Cmax). The drugs were considered bioequivalent if the 90% confidence intervals (CI) of the T/R geometric mean ratios for Cmax and AUC0-t were in the range of 80-125%. Safety assessment included analysis of vital signs, physical examination, laboratory tests, 12-lead electrocardiography (ECG), and registration of adverse events (AEs) during the study.
Results. Of the 46 randomized volunteers, 44 comprised the safety population. Forty two participants completed the study without significant protocol deviations and comprised the population for pharmacokinetic, statistical analysis and bioequivalence. The values of pharmacokinetic parameters T and R were comparable. The 90% CIs for Cmax and AUC0-t were within the acceptable bioequivalence range of 80,00-125,00% as follows: 91,71-107,41% and 91,58-115,83%, respectively. A total of 2 AEs were recorded in 1 participant after receiving the reference drug. The frequency of AEs did not differ between the groups. No clinically significant deviations in vital signs, physical examinations, laboratory tests, or ECG data were observed in either group during the study.
Conclusion. T and R were considered bioequivalent and demonstrated similar safety profiles.
CLINICAL GUIDELINES
Russian Society of Cardiology (RSC)
With the participation of: All-Russian Scientific Society of Specialists in Clinical Electrophysiology, Arrhythmology and Pacing (VNOA), the Association of Cardiovascular Surgeons
Approved by the Research and Practical Council of the Ministry of Health of the Russian Federation
Announcements
2025-09-04
Публикация статей до конца года
У нас полностью сформированы номера до конца 2025 года. Мы ограниченно можем принять в номера 11 и 12-2025 статьи с оплатой срочной публикации (Fast Track) только для статей, которые уже прошли рецензирование или пройдут рецензирование до 30 октября.
2025-08-29
Обработка персональных данных
С 1 сентября 2025 года вступают в силу поправки в ч. 1 ст. 9 Закона № 152-ФЗ, которыми вводится новое требование к согласию на обработку персональных данных. Согласие должно быть оформлено отдельно от информационных и (или) иных документов, которые подписывает субъект персональных данных (Федеральный закон от 24 июня 2025 года №156-ФЗ).
2025-06-15
Список принятых статей, запланированных на ближайшие номера
Уважаемые авторы, вывешиваем список статей, работа над которыми будет вестись в течение лета (список будет пополняться и изменяться)
2025-06-01
Уточнения в «Правила для авторов» в отношении рисунков
Уважаемые авторы!
Журнал вносит уточнения в «Правила для авторов» в отношение рисунков, которые предоставляются при подаче статьи для рассмотрения к публикации.
2025-02-21
Тематические номера Российского кардиологического журнала в 2025 году
номер 10-2025. Генетические аспекты кардиологии
Ответственный редактор: Никулина С. Ю. (Красноярск)
номер 12-2025. Достижения российской кардиологии 2025
Ответственный редактор: статьи выбираются редакцией журнала.
Дополнительные выпуски: "Клинические случаи" (июнь, ноябрь), "Обзоры литературы, мнения по проблеме" (июнь, ноябрь), "Диссертационные статьи" (июнь, ноябрь)
2025-02-16
Тематика номеров РКЖ. Образование в 2025 году
| More Announcements... |

ISSN 2618-7620 (Online)











































