



ORIGINAL ARTICLES

- Based on the results of the analysis of discharge summary and death certificates of patients with HF, data laboratory and instrumental assessment meet the criteria for the quality of medical care in most cases, with the exception of the lack of determination of natriuretic peptides.
- Triple therapy for HF with low and moderately reduced EF, if indicated, was prescribed to only 54,1% of patients.
- An incomplete presentation of recommendations in the discharge summary was identified, including very low of proportions summaries (10%) with the data of outpatient visit after discharge (within the first 14 days).
Aim. To assess the compliance of the management of patients with heart failure (HF) with quality criteria (QC) for health care, including discharge instructions for patients.
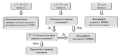
Material and methods. Hospitalizations of patients aged over 18 years with HF (ICD 10 code — I50.x) during the period from January 1, 2019 to October 1, 2020 were randomly selected from the "Chronic Heart Failure" registry of St. Petersburg. Discharge and post-mortem summaries were assessed for compliance with the quality criteria listed in the 2020 Russian Chronic Heart Failure guidelines.
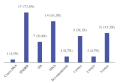
Results. The study included 553 patients (women, 71,1%, mean age, 82,0±9 years, comorbidities: hypertension — 99,1%, coronary artery disease — 97,6%, chronic kidney disease — 53,2%, diabetes — 32,6%). Electrocardiography (QC № 1) was performed in 94,2% of patients, chest radiography (QC № 2) 91,7%, echocardiography (QC № 3) — 81,0%, but the results were not always informative. The exact ejection fraction (EF) value was reported in 55,4% of patients. Laboratory examination corresponded to QC № 4-6 in 20,3% of cases and was performed in 53,3-94,9%. Natriuretic peptides (NPs) were not determined (QC № 7-0%).
The completeness of intravenous therapy (QC № 8) was not assessed due to insufficient physical examination data.
Oral therapy (QC № 9) was prescribed frequently as follows: renin-angiotensinaldosterone system inhibitors (RAASo) — 93,3%, beta blockers (BBs) — 85,4%, mineralocorticoid receptor antagonists (MRAs) — 78,7%. However, triple RAAS+BB+MRA therapy was carried out in 54,1% of HF cases with EF <50% and no contraindications.
Diet was recommended in 87,1% of summaries, water-salt regimen — 53,3%, drug titration — 8,2%. The date of visit to outpatient cardiologist was indicated in 10,0%.
Conclusion. With the exception of NP assessment, the scope of paraclinical studies corresponded to the QC in the majority of patients. Optimal therapy was prescribed to 54,1% of patients with EF <50%. An early outpatient visit after discharge was indicated in 10,0% of summaries.

What is already know about the subject
- In multi-level or diffuse coronary artery disease, the measurement of the instantaneous wave-free ratio (IFR) makes it possible to assess the functional significance of each lesion separately. This feature of the method is the basis of the virtual stenting technology, which makes it possible to predict the physiological effect of percutaneous coronary intervention.
Results of the study
- A high correlation was demonstrated between the predicted value of the iFR obtained using the virtual stenting technology and the actual value of the iFR achieved after stent implantation.
- iFR mapping and virtual stenting technology make it possible to revise the angiographic classification of lesions by extent, which leads to a statistically significant reduction in the number of implanted stents and the length of the stented segment.
Aim. To evaluate the accuracy of virtual stenting in predicting the physiological effect of percutaneous coronary intervention (PCI) for multilevel coronary artery disease (CAD).
Material and methods. In order to define PCI strategy, 34 patients with multilevel CAD underwent assessment of instantaneous wave-free ratio (iFR) with mapping. Using the virtual stenting, predicted iFR (priFR) was assessed. After stent implantation, the factual iFR (fiFR) was re-assessed. A discrepancy between the priFR and fiFR by 0,03 was considered the threshold level of a significant difference and "poor agreement" criterion between measurements.
Results. Mean iFR before PCI was 0,77±0,11; after PCI, this indicator increased significantly and amounted to 0,94±0,04 (p<0,001). Comparison of the predicted and factual iFR revealed that the difference did not significantly depend on the value (rxy=-0,183; p=0,300), and mean difference between measurements was 0,013 (standard deviation, ±0,019), which indicates no systematic discrepancy and good comparability of the studied methods. In addition, correlation analysis of priFR and fiFR revealed a significant strong (Chaddock scale) direct relationship (r=0,854; p<0,001). Independent predictors of "poor agreement" were heart rate and systolic blood pressure before surgery. Discrepancy in decisions on the choice of stented lesions and the required number of stents based on coronary angiography (CAG) and MRI occurred in 21 patients (62%) and 16 patients (47%), respectively. After iFR measurement, there was a significant decrease in the mean length of affected segment (from 61,82±19,68 mm (CAG) and 49,15±19,19 mm (iFR)), which made it possible to significantly reduce the number of implanted stents from 1,91±0,57 (CAG) to 1,50±0,56 (p=0,001).
Conclusion. Mapping the iFR and virtual stenting technology makes it possible to revise the classification of coronary lesions by length, which leads to a significant reduction in the number of implanted stents and the length of stented segment. High correlation between priFR and fiFR achieved in our study indicates the high accuracy of virtual stenting in predicting the physiological effect of stenting.

- The Ross procedure has excellent long-term outcomes such as survival, freedom from stroke and bleeding. However, some patients require valve reinterventions.
- The main reason for reoperations is aortic regurgitation, most often due to neoaortic dilatation.
- Modified methods aimed at preventing this complication show promising results.
Aim. To analyze the immediate outcomes of reinterventions after Ross procedure.
Material and methods. From April 2009 to December 2022, 224 Ross operations in adults were performed at the Federal Center for Cardiovascular Surgery. The retrospective study included 17 patients who required repeated interventions (14 men/3 women). The mean age of the patients was 38±11 years, with a minimum age of 21 and a maximum of 54 years. A history of infective endocarditis was revealed in 4 (23,5%) patients, hypertension — in 3 (17,6%) patients. Of the 17 included patients, 15 patients underwent the classic Ross operation ("full root replacement"), while 2 — a modified technique (1 — wrapping with aorta, 1 — wrapping with a Dacron graft). Annulus enhancement was previously performed in 3 patients.
Results. Interventions on the pulmonary autograft and homograft were performed in 16 and 4 cases, respectively. The main indication for pulmonary autograft intervention was aortic regurgitation in 15 cases, and neoaortic aneurysm in 14 cases. In 3 patients, there was pulmonary homograft stenosis, while in 1 case — thrombosis. Two patients required interventions on other valves: 1 — mitral valve stenosis, 1 — severe tricuspid regurgitation. Mean reoperation, cardiopulmonary bypass and myocardial ischemia time were 289±62, 126±35 and 98±22 min, respectively. Combined interventions were performed in 6 cases. David valve-sparing procedure was performed in 9 patients, Bentall-de Bono technique — in 3, aortic valve repair — in 2, mechanical aortic valve replacement — in 2, supracoronary ascending aorta replacement — in 2, pulmonary homograft replacement — in 2, pulmonary homograft thrombectomy — in 1, pulmonary homograft repair — in 1 patient, mitral valve replacement — in 1 patient, tricuspid valve repair — in 1 patient. One patient required resternotomy for bleeding. There were no postoperative complications (perioperative myocardial infarction, acute kidney injury, stroke, sternal infection, cardiac tamponade) and deaths. The median length of stay in intensive care unit was 21 [16-23] hours.
Conclusion. Reoperations after the Ross procedure may be required for different pathologies, but all can be performed surgically with a high safety in experienced operator.
- The important role of a differentiated approach in screening for familial hypercholesterolemia has been shown.
- Diagnostic criteria for familial hypercholesterolemia do not take into account the estrogen status of women who are potential carriers of pathological mutations.
Aim. To analyze the prognostic value of the Dutch Lipid Clinic Network (DLCN) and Simon Broome Register (SBR) screening criteria for familial hypercholesterolemia (FH) in men and women with dyslipidemia.
Material and methods. The study included 1233 patients with dyslipidemia.
Biomaterial samples from 421 patients were studied using Next Generation Sequencing (NGS) to identify FH-associated genes. Statistical analysis was carried out using the StatTech v program. 3.1.6 (OOO Stattekh, Russia).
Results. The most significant factors for predicting the FH in men are the level of low-density lipoprotein cholesterol (LDL-C) (1,77 times), positive family history for coronary artery disease (CAD) (6,26 times), multivessel coronary artery disease (4,05 times); in women before menopause — LDL-C (1,77 times per 1 mmol/l) and/or family history of coronary artery disease (3,31 times), in menopausal women — total cholesterol level (1,79 times per 1 mmol/l), coronary artery disease (6,52 times) and/or family history of stroke (6,04 times), xanthomas (4,24 times). Acute myocardial infarction and/or coronary stenting, arcus senilis, extracranial artery atherosclerosis did not prove to be prognostically significant for FH diagnosis.
Conclusion. Diagnostic criteria for potential FH vary among patient populations. Its diagnostic significance depends on sex, and in women, reproductive status.
- Due to the lack of randomized clinical trials conducted among patients with ST-segment elevation myocardial infarction (STEMI) over 90 years of age, invasive tactics are chosen less frequently than in younger patients.
- The results obtained in our study indicate the advantage of invasive management tactics for patients with STEMI over the age of 90 years.
- At the moment, there is no consensus on the absolute advantage of an invasive treatment strategy in elderly and long-lived patients. Therefore, it is advisable to conduct a prospective study that will provide reliable information about the choice of the optimal approach.
Aim. To evaluate the effectiveness and safety of an invasive approach in patients with ST-segment elevation myocardial infarction (STEMI) aged 90 years and older.
Material and methods. This retrospective single-center study was conducted at the V. P. Polyakov Samara Regional Clinical Cardiology Dispensary. In 20132020, 104 patients aged 90 years and older were hospitalized with a diagnosis of STEMI. The mean age of patients was 91,7 years (90-100), while the proportion of women was 67,3%. Patients included in the analysis were divided into groups of conservative treatment (n=81, mean age, 91,9 (90-100) years, women 70,4%) and invasive management (coronary angiography + percutaneous coronary intervention (PCI)) (n=23, mean age, 91,0 (90-94) years, women, 56,5%).
Results. The groups were comparable in basic characteristics. In-hospital mortality in the conservative strategy group was 48,1% vs 17,4% in the invasive management group (p=0,009; odds ratio (OR) 3,35; 95% confidence interval (CI) 1,23-9,15). During the first year after discharge, 25,9% (n=21) died in the conservative strategy group and 30,4% (n=7) in the invasive strategy group (p=0,79; OR 0,85; 95% CI 0,42-1,75). In total (during the hospitalization period and within 1 year after discharge), 60 people (74,1%) died in the conservative strategy group, while in the invasive treatment group — 11 (47,8%) (p=0,02; OR 3,11; 95% CI 1,19-8,11). Life expectancy in patients with STEMI aged 90 years and older after discharge from hospital was 83,95 days for the conservative strategy group and 103,85 days for the invasive strategy group (p=0,67).
Conclusion. The data obtained in our study support primary PCI as a treatment strategy for patients with STEMI aged 90 years and older.
- The effect of rehabilitation in patients after hospitalization with COVID-19 pneumonia on cardiovascular endpoints after 1 year was shown.
- Telerehabilitation after COVID-19 reduces the risk of cardiovascular mortality after 1 year, but does not affect the incidence of other endpoints.
- Both rehabilitation options reduce the incidence of cardiovascular hospitalization compared with no rehabilitation.
Due to the large number of complications and decreased quality of life after coronavirus disease (COVID-19), physical and psychological rehabilitation of patients is relevant. However, the effectiveness of rehabilitation on endpoints has not yet been demonstrated.
Aim. To determine the effectiveness of different rehabilitation options in hospitalized patients with COVID-19 on the development of long-term adverse cardiovascular events 1 year after discharge.
Material and methods. In a single-center, non-randomized observational study, 3 groups of patients were formed after hospitalization with COVID-19: I — with telemedicine rehabilitation (n=118), II — with rehabilitation in a specialized department (n=46) and III — without rehabilitation (n=175). After 1-year followup, groups were compared regarding following endpoints: cardiovascular mortality, myocardial infarction, stroke, pulmonary embolism, atrial fibrillation and cardiovascular hospitalization. Propensity score matching analysis was used to optimize differences between comparison groups.
Results. Rehabilitation after hospitalization of patients with COVID-19, both in the hospital and remotely for 1 year, helps to reduce cardiovascular hospitalization rate. In addition, remote rehabilitation reduces cardiovascular mortality.
Conclusion. Both rehabilitation options reduce the incidence of cardiovascular hospitalization compared to no rehabilitation.
GUIDELINES REVIEWS
The novelty of the 2023 National Guidelines for Lipid Metabolism Disorders is presented regarding the categorization of cardiovascular risk, target and optimal levels of blood lipids, diagnosis and therapeutic approaches to the treatment of dyslipidemia.

This year, new domestic recommendations for assessing and correcting the risk of cardiac complications during non-cardiac surgery have been published. These guidelines provide simple and practical key messages to facilitate decision-making in real-life clinical practice. The proposed algorithm for the management of patients before non-cardiac operations, focused on integral risk assessment, assessment of functional status and biomarkers. This review provides a summary of perioperative drug therapy, management of the most common CVDs, and focuses on specific care based on the risk of the patient's preexisting clinical conditions. Finally, the document includes practical recommendations for the management of postoperative complications, and also includes a new section on perioperative myocardial infarction/injury.
CLINICAL CASES

- The presence of a pacemaker is a risk factor for pulmonary embolism.
- Conservative management of pacemaker infective endocarditis is ineffective. Sepsis plays the role of a trigger for hypercoagulation.
- In case of distal pulmonary artery involvement and technical feasibility, staged balloon pulmonary angioplasty with pre- and postoperative personalized therapy is advisable.
A case report is devoted to the successful management of a 33-year-old patient with subacute infective endocarditis of the tricuspid valve and pacemaker, as well as chronic thromboembolic pulmonary hypertension. There were following therapy stages: 1) pharmacotherapy — antimicrobial agents, treatment of heart failure, pulmonary hypertension; 2) an interventional approach — tricuspid valve replacement with chamber sanitation, pacemaker explantation, endocardial lead removal from the right heart, implantation of a pacemaker with an epicardial lead system and 3) delayed balloon pulmonary angioplasty.

- Computed tomography angiography of the thoracic aorta, extracranial arteries and coronary bypass grafts in patients with left subclavian artery occlusion after myocardial revascularization is key for the correct diagnosis of coronary subclavian steal syndrome.
- Carotid-subclavian bypass is the most effective approach to the treatment of coronary subclavian steal syndrome.

- In a patient with Takotsubo syndrome, left ventricular apical dyskinesia was initially detected; no local contractility disturbances were detected over time using echocardiography.
- Left atrial strain reservoir (LASr) can be used to characterize the communication of left and right heart.
Among various diagnostic methods, echocardiography (EchoCG) is most often used to identify Takotsubo syndrome. Left ventricular apical ballooning and the absence of permanent local contractility disturbances makes it possible to confirm the diagnosis. Currently, the available literature provides insufficient data on longitudinal strain (LS) of various cardiac chambers in this condition. The current case report demonstrates complete restoration of left heart LS within 1 month with its initial significant decrease.
REVIEW
- The post-pulmonary syndrome can affect substantially the quality of life.
- To improve the overall health outcomes of patients with acute pulmonary embolism (PE), adequate measures to diagnose it and strategies to prevent long-term outcomes of PE are essential.
- To evaluate safety and patient reported outcome measures (PROM) on outpatient treatment of acute PE.
- The majority of PPES patients are ultimately diagnosed with post-PE functional impairment and utilizing PROMs (can be helpful in objectively assessing complains after acute PE, in order to further evaluate and optimization their
People who survive an episode of pulmonary embolism have an increased risk of developing chronic complications despite curative anticoagulant treatment. The association of dyspnoea, low functional capacity, right heart failure, chronic thromboembolic pulmonary hypertension, or chronic thromboembolic pulmonary disease is part of the notion of post-pulmonary embolic syndrome (PPES). The symptoms can be limiting, substantially affecting the quality of life. To improve the overall health outcomes of patients with acute pulmonary embolism, adequate measures to diagnose it and strategies to prevent long-term outcomes of pulmonary embolism are essential.
The objective of this study is to provide a definition of PPES and review the most recommended patient-reported outcome measures (PROMs) for assessing the functionality of these patients.
We searched PubMed for papers from the last 5 years that contain the terms: postpulmonary embolism syndrome; symptoms; PROMs; score; quality of life; dyspnea. Repetitive publications were excluded. The data from the publications have been summarized in this descriptive overview.
Hypertension (HTN) is widespread among middle-aged and elderly people, including those doing sports. For the first time in 2020, the European Society of Cardiology guidelines on sports cardiology and exercise in patients with cardiovascular disease included adult and elderly patients in a separate group. However, this is a heterogeneous category of patients, including everyone over 35 years of age. Therefore, admittance of athletes to training and competitions still remains at the discretion of physician.
Aim. To assess the relationship and mutual influence of hypertension, other cardiovascular risk factors and sports in middle-aged and elderly people.
Material and methods. Our narrative review is based on 50 articles published on Pubmed, Scopus, Web of Science and eLIBRARY.ru, selected using the keywords "veteran athletes", "arterial hypertension", "cardiovascular risk", "physical activity". Related papers over the past 5 years were evaluated.
Results. Currently, there is a trend toward an increase in the number of veteran athletes whose problems are not reflected in guidelines on sports and exercise.
Conclusion. In the future, large randomized studies are needed to assess the response of blood pressure (BP) to intense exercise, as well as to determine the normal BP response and clear strategy to manage this category of people, depending on the presence of hypertension.
INFORMATION

ISSN 2618-7620 (Online)












































